













 7 / 17
7 / 17

Page 97
May 24-25, 2018
London, UK
Vascular Surgery 2018
3
rd
Edition of World Congress & Exhibition on
Vascular Surgery
Journal of Vascular and Endovascular Therapy
ISSN: 2573-4482
Introduction:
Given the high mortality rate in patients with type A
aortic dissection, predictive tools to identify patients at increased
risk of aortic dissection, when the diameter of ascending aorta is
still under the threshold of 55 mm, are needed to assist clinicians
for optimal intervention and to help patients raise their alert.
Method:
We evaluated 528 consecutive patients of acute type
A aortic dissection (AAAD) admitted to Fuwai Hospital, Beijing,
China between 2009 and 2013. Univariate testing followed by
multivariate logistic regression analysiswas performed to identify
independent predictors of AAAD at a diameter less than 55 mm.
A simplified scoring system for predicting aortic dissection at a
smaller diameter was then established based on the results of the
multivariate analysis.
Results:
Of the528AAADpatients, 375 (71%)werewithadiameter
less than 55 mm at the level of ascending aorta. A total of 25
variables as regard with demographic characteristics, clinical
features and imaging were investigated. Logistic regression
identified the following presenting variables as predictors of AD
at a diameter less than 55 mm: age≥50 years (OR, 0.41; 95% CI,
0.26 to 0.65; P<0.01), hypertension (OR, 2.02; 95%CI, 1.20 to 3.40;
P=0.01), history of aortic valve replacement (OR, 0.05; 95% CI,
0.01 to 0.42; P=0.01), history of catheterization (OR, 7.45; 95% CI,
1.26 to 44.21; P=0.03), hepatic cyst (OR, 2.69; 95%CI, 1.30 to 5.60;
P=0.01), renal cyst (OR, 3.62; 95% CI, 1.85 to 7.08; P<0.01), bovine
arch (OR, 6.39; 95% CI, 1.47 to 27.90; P=0.02), BAV (OR, 0.19; 95%
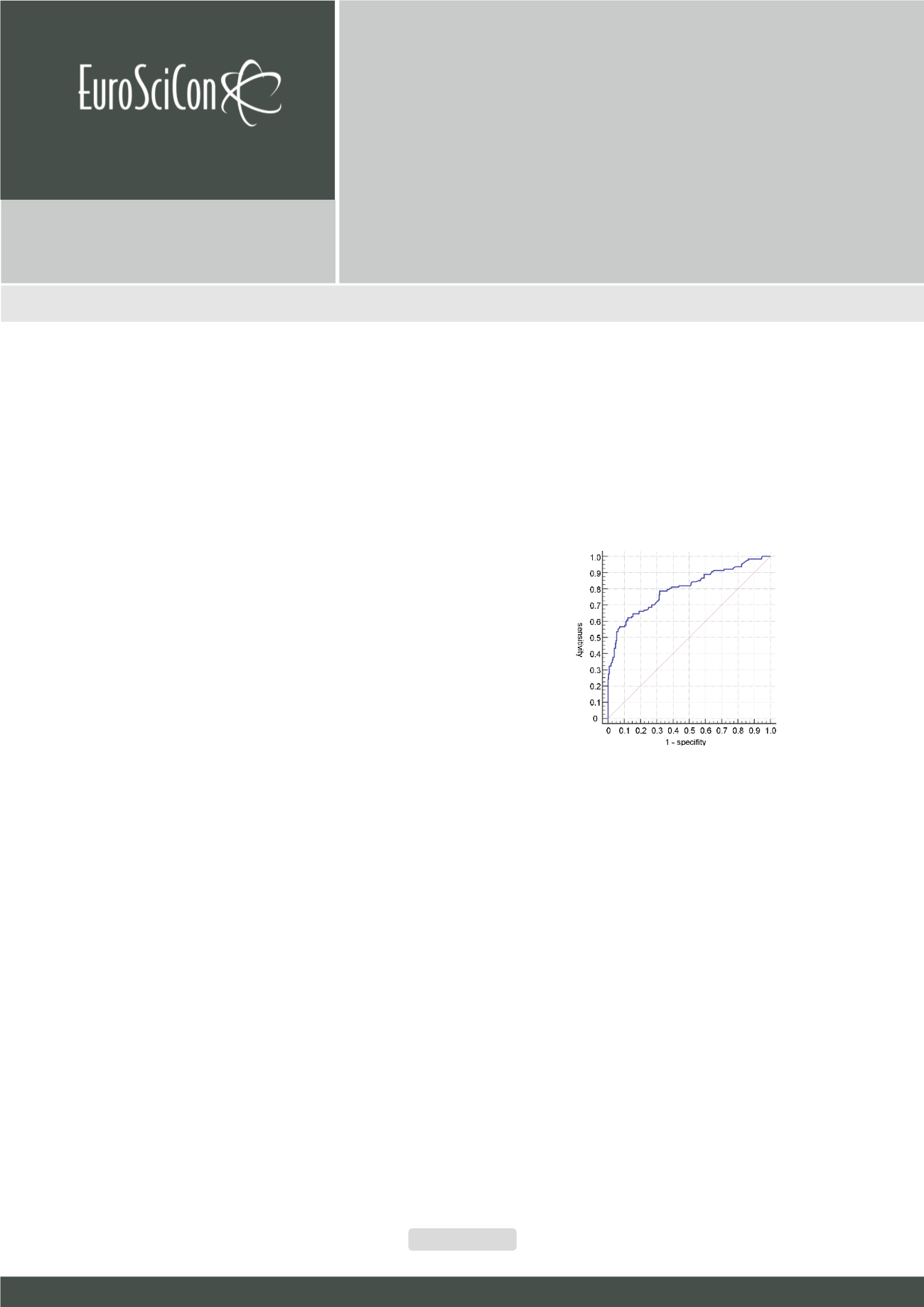
CI, 0.04 to 0.95; P=0.04). Area under the receiver operating curve
(ROC) was 0.73. Hosmer-Lemeshow statistic, P=0.28.
Conclusion:
Patients with age <50 years, hypertension, a history
of catheterization, hepatic cyst, renal cyst, or bovine arch were
more likely to develop aortic dissection at a smaller diameter.
Recent Publications
1. Cheng L, Huang F, Chang Q, Zhu J, Yu C, Liu Y, et al.
(2010) Repair of extensive thoracoabdominal aortic
aneurysm with a tetrafurcate graft: midterm results
of 63 cases. The Heart Surgery Forum 13(1):E1-6.
2. Sun X, Zhang L, Yu C, Qian X and Chang Q (2014)
One-stage repair of extensive aortic aneurysms: mid-
term results with total or subtotal aortic replacement.
Interactive Cardiovascular &Thoracic Surgery 18(3):278-
82.
3. Zhang L, Yu C, Qian C, Luo X, Qiu J and Liu S (2016)
Comparison of gene expression profiles in aortic
dissection and normal human aortic tissues. Biomedical
Reports 5(4):421-7.
4. Liu P, Qian C, Qian X, Sun X, Yu C, Tian C, et al. (2016)
Early and mid-term results after hybrid total arch repair
of DeBakey type I dissection without deep hypothermic
circulatory arrest. Interactive Cardiovascular & Thoracic
Surgery 23(4):608.
Biography
Cun Tao Yu is one of the most famous cardiovascular surgeons in China.
He is especially good at all kinds of operation of large vessels and has com-
pleted over 1500 operations such as total arch replacement and thoracoab-
dominal aortic replacement. Jin Lin Wu is his doctoral candidate.
jinlinhorsy@outlook.comPossible predictors of aortic dissection at a diameter less
than 55 mm
Jin Lin Wu
and
Cun Tao Yu
Peking Union Medical College(PUMC), China
Jin Lin Wu et al., J Vasc Endovasc Therapy 2018, Volume 3
DOI: 10.21767/2573-4482-C1-003
Figure 1:
ROC curve to evaluate the predictive power of the multivariate analysis.