













 12 / 17
12 / 17

Page 102
May 24-25, 2018
London, UK
Vascular Surgery 2018
3
rd
Edition of World Congress & Exhibition on
Vascular Surgery
Journal of Vascular and Endovascular Therapy
ISSN: 2573-4482
Mycotic abdominal aortic aneurysm (MAAA) is a rare but life-
threatening condition with an incidence of about 0.65-2% of all
aortic aneurysms. MAAA have poor prognosis as they have
tendency to grow rapidly and rupture and the patients often
have severe comorbidities and coexisting septic conditions.
Conventional surgical treatment is open surgery but is associated
with high morbidity and mortality and can be very demanding or
even impossible. Endovascular aneurysm repair (EVAR) is a less
invasive but controversial alternative to conventional open repair
ofMAAA. Amajor disadvantageof EVAR is that the infected tissue,
including the aneurysm itself, is not resected, whichmay facilitate
reinfection, recurrent sepsis, and infection of the endoprosthesis.
Methodology: Three cases of MAAA are described; all treated
with endovascular stent graft with variable configurations (2
cases treatedwith EVAR and 1with surgeonmodified Fenestrated
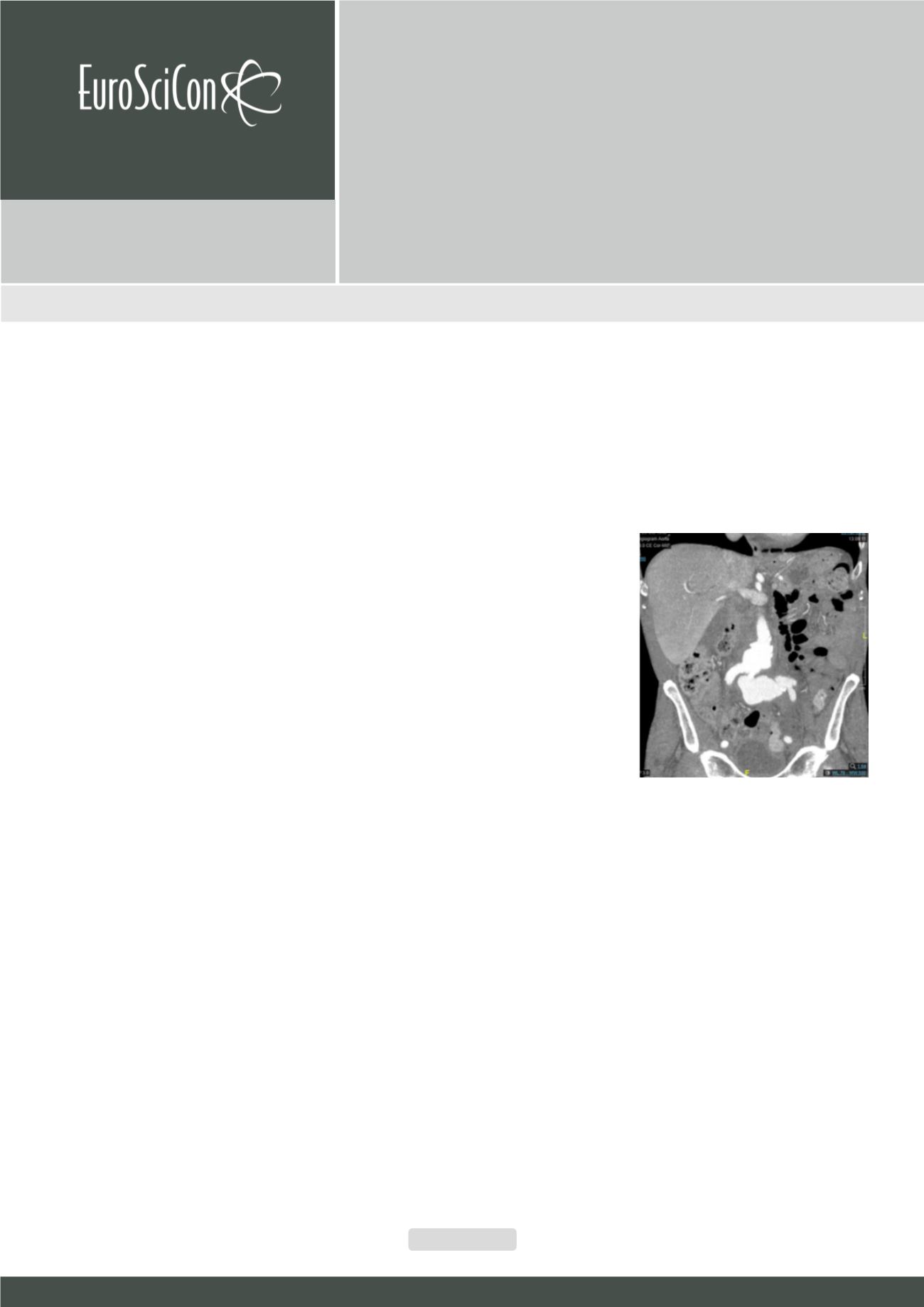
EVAR). The clinical diagnosis of MAAA, was made by clinical
presentation, results of hematologic tests and culture, and CT
findings. All cases grew streptococcus pneumoniae on blood
culture. All patients underwent successful placement of stent
grafts for their aneurysms. All patients were given antibiotics
preoperatively and postoperatively, initially with broad-spectrum
antibiotics intravenously and later, when discharged from the
hospital, oral treatment guided by culture results, when available.
Antibiotic therapy was administered after consultation with
infectious disease specialists. No 30-day postoperative mortality
was observed. Conclusion: Our short- term review shows that
repair of MAAA can be accomplished with endovascular repair.
This may be a safer alternative to open repair particularly in
patients who are not suitable for conventional open repair.
Recent Publications
1. Reddy D J, Shepard A D, Evans J R, Wright D J, Smith
R F, Ernst C B (1991) Management of infected aortoiliac
aneurysms. Arch Surg 126: 873 – 879.
2. Muller B T, Wegener O R, Grabitz K, Pillny M, Thomas L,
Sandmann
W
(2001) Mycotic
aneurysms of
the
thoracic
and abdominal
aorta
and
iliac
arteries:
experience with
anatomic and
extra anatomic
repair in 33
cases. J Vasc
Surg 33: 106 –
113.
3. Fillmore A J,
Valentine R J (2003) Surgical mortality in patients with
infected aortic aneurysms. J Am Coll Surg 196: 435 –
441.
4. Hsu R B, Chen R J, Wang S S, Chu S H (2004) Infected
aortic aneurysm: clinical outcome and risk factor
analysis. J Vasc Surg 40: 30 - 35
5. Sorelius K, Mani K, Bjorck M, Nyman R, Wanhainen A
(2009) Endovascular repair of mycotic aortic aneurysms.
J Vasc Surg 50: 269 – 274.
Biography
Sanjay Singh has expertise and passion in vascular and endovascular sur-
gery. He has done complex aortic endovascular fellowship and is a vascular
consultant working in United Kingdom. His open and contextual surgical
techniques are based on researched and practiced models which help cre-
ate new pathways for innovation. He has achieved this aptitude after years
of experience in research and teaching in University hospitals and institu-
tions. The ever-responsive and adapting field of endovascular surgery has
improved the survival rates of high risk patients.
dr_sanjaysingh@hotmail.comEndovascular Management of Mycotic Abdominal Aortic
Aneurysm Secondary to Streptococcal Pneumoniae
Sanjay Singh, Muhammad Usman Cheema, Asghar Butt
and
Nityanand Arya
United Lincolnshire Hospitals NHS Trust, UK
Sanjay Singh et al., J Vasc Endovasc Therapy 2018, Volume 3
DOI: 10.21767/2573-4482-C1-003