













 3 / 17
3 / 17

Page 93
May 24-25, 2018
London, UK
Vascular Surgery 2018
3
rd
Edition of World Congress & Exhibition on
Vascular Surgery
Journal of Vascular and Endovascular Therapy
ISSN: 2573-4482
Internal carotid artery aneurysm open repair without
mandibular subluxation: a case report
Rezende A N C A, Pitta C A, Manzioni R, Portela L D A
and
Sotelo F J B
Ipiranga Hospital, Brazil
Rezende A N C A et al., J Vasc Endovasc Therapy 2018, Volume 3
DOI: 10.21767/2573-4482-C1-003
E
xtracranial carotid artery aneurysms (ECCAs) are rare, with an
estimated incidence of less than 1%. They can have different
etiologies: atherosclerotic (main etiology), dysplastic, infectious,
inflammatory and post-traumatic. The diagnosis can be made
by CT-angiogram, but the gold-standard is digital subtraction
angiography. Their treatment, not yet been well established, can
be open repair, which is a safe surgical option with low prevalence
of complications (mostly cerebral ischemia) endovascular
repair, or conservative. Most open repairs require submandibular
subluxation, because of the site of the aneurysm. We describe
the case of a 61-year-old white woman with a cervical bulging,
pulsatile at the physical exam, and occipital headache. CT
angiogram showed: signs of dissection of right vertebral artery
and a fusiform aneurysm dilatation of the left internal carotid
artery. Since patient had two different types of lesions in two
different artery sites, the possibility of fibromuscular dysplasia
was consideredas adifferential diagnosis. Since the kinkingmade
endovascular repair unfavorable tobedone, open repairwasopted
and an aneurysm resection was carried out, with primary end-to-
end anastomosis of the internal carotid artery with the internal
carotid artery. During the surgical procedure, it was noticed
that, because of the location and kinking of the aneurysm, the
mandibular subluxation wasn’t necessary (an uncommon feature
for this type of surgery). The products of the biopsy specimen
were cultured and analyzed histo and anatomopathologically
which subsequently excluded the possibility of FMD.
Recent Publications
1. Jiber H, Zrihni Y, Naouli H and Bouarhroum A (2017)
Fibrodysplasic aneurysms of the extracranial internal
carotid artery: a new case report. Pan Afr Med J. 28:170.
2. Jin C, Hu Z and He Y (2017) A wide-necked extracranial
internal carotid artery saccular aneurysm with ipsilateral
proximal compression. J Clin Ultrasound 45(2):116-120.
3. YamamotoS,AkiokaN,KashiwazakiD,KohM,Kuwayama
N and Kuroda S (2017) Surgical and endovascular
treatmentsofextracranialcarotidarteryaneurysms-report
of six cases. J Stroke Cerebrovasc Dis. 26(7):1481-1486.
4. Hongo H, Inoue T, Tamura A and Saito I (2017) Surgical
strategy to minimize ischemia during trapping/resection
of giant extracranial carotid artery aneurysmstratified by
collateral evaluation. Surg Neurol Int. 8:28.
5. Guzhin V E, Dubovoy A V and Cherepanov A V (2016)
Surgical treatment of distal extracranial internal carotid
artery aneurysms associated with pathological artery
kinking. Zh Vopr Neirokhir ImN N Burdenko. 80(5):62-66
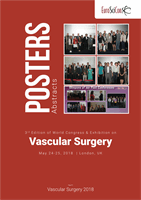
Figure 1:
End-to-end
anastomosis (c) of the ICA.
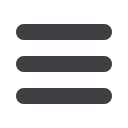
Figure 3:
CT angiogram — left
interior carotid aneurysm
(red arrow); vertebral artery
dissection (blue arrow)..
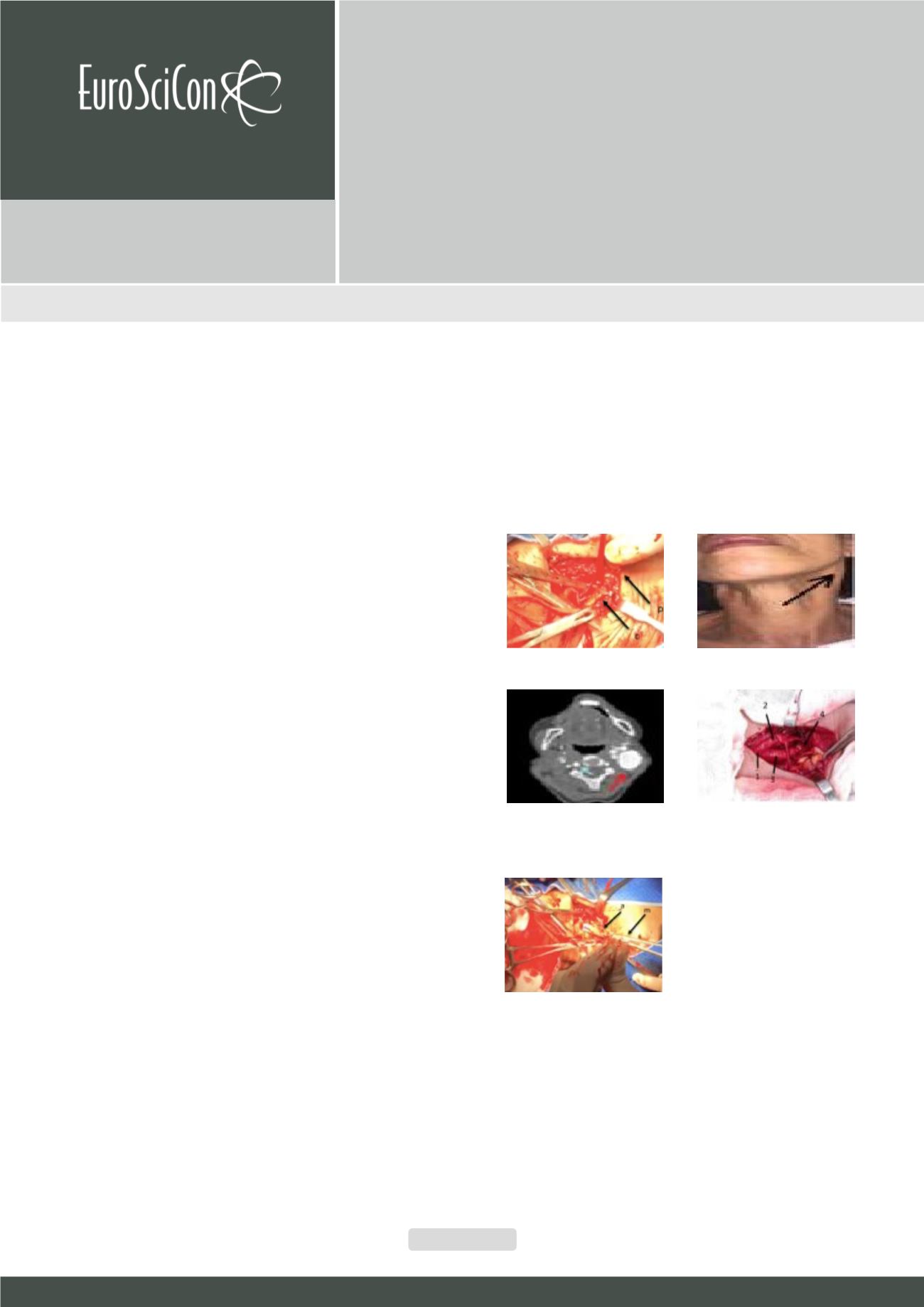
Figure 5:
Partial resection of the aneurysm (a -
aneurysm; m- metzenbaum)
Figure 2:
Patient’s bulging on left
cervical area 2 (arrow).
Figure 4:
Internal carotid
aneurysm shown after
dissection (1 = common carotid
artery (CCA); 2 = external
carotid artery (ECA); 3 = internal
carotid artery (ICA); 4 = post
anastomotic ICA)