













 10 / 17
10 / 17

Vascular Surgery 2019
Journal of Vascular and Endovascular Therapy
ISSN: 2573-4482
Page 66
March 28-29, 2019
Rome, Italy
Vascular Surgery
4
th
Edition of World Congress & Exhibition on
Ziyan Kassam, J Vasc Endovasc Therapy 2019, Volume 4
DOI: 10.21767/2573-4482-C1-006
Happily EVAR after? – The truth about EVAR
Ziyan Kassam
King’s College London, United Kingdom
E
ndovascular aneurysm repair (EVAR) for abdominal
aortic aneurysm(AAA) repair has been responsible for
a seismic shift in themanagement of AAAs. Compared to
traditional open surgical repair (OSR), EVAR is associated
with significantly a improved peri-operativemorbidity and
mortality. As the technology and applications of EVAR
continue to evolve, so does the literature investigating
its outcomes. Recently, longer-term follow-up results of
randomised controlled trials (RCTs) comparing EVAR and
OSR have been published. In light of this new evidence,
this review aimed to evaluate the long-term outcomes
from such prospective multi-centre RCTs, assessing the
effectiveness, advantages and disadvantages of EVAR
and OSR, in terms of endograft-related complications, re-
intervention rates, and longer-termmortality, todetermine
whether EVAR really is the better option. Following
evaluation of the results, the early survival benefit of
EVAR is not sustained, with longer-term life expectancy
remaining poor regardless of operative modality.
Additionally, the development of technical EVAR-related
post-operative complications, predominantly endoleaks,
stent-graft migration and stent-limb thrombosis requires
further corrective re-intervention. Thus, lifelong imaging
surveillance is crucial to determine the occurrence of
such events, and plan timely intervention to prevent
secondary sac rupture. However, this results in EVAR
being costlier over a patient’s lifetime when compared to
OSR. Despite the choice between OSR and EVAR for AAA
repair remaining an individualised clinical decision, there
is a greater tendency to choose EVAR, predominantly
due to increased surgeon familiarity. Data from long-
term trials however are based on initial EVAR device
generations, thus newer stent-grafts are likely to improve
safety and expand their applicability. As a result, further
long-term RCTs are warranted to compare the relative
benefits and disadvantages of modern EVAR devices.
Recent Publications
1. Brown L C, et al. (2004) The UK endovascular
aneurysm repair (EVAR) trials: design,
methodology and progress. European Journal
of Vascular and Endovascular Surgery
27(4):372-381.
2. Prinssen M, Buskens E and Blankensteijn J D
(2002) The Dutch randomised endovascular
aneurysm management (DREAM) trial:
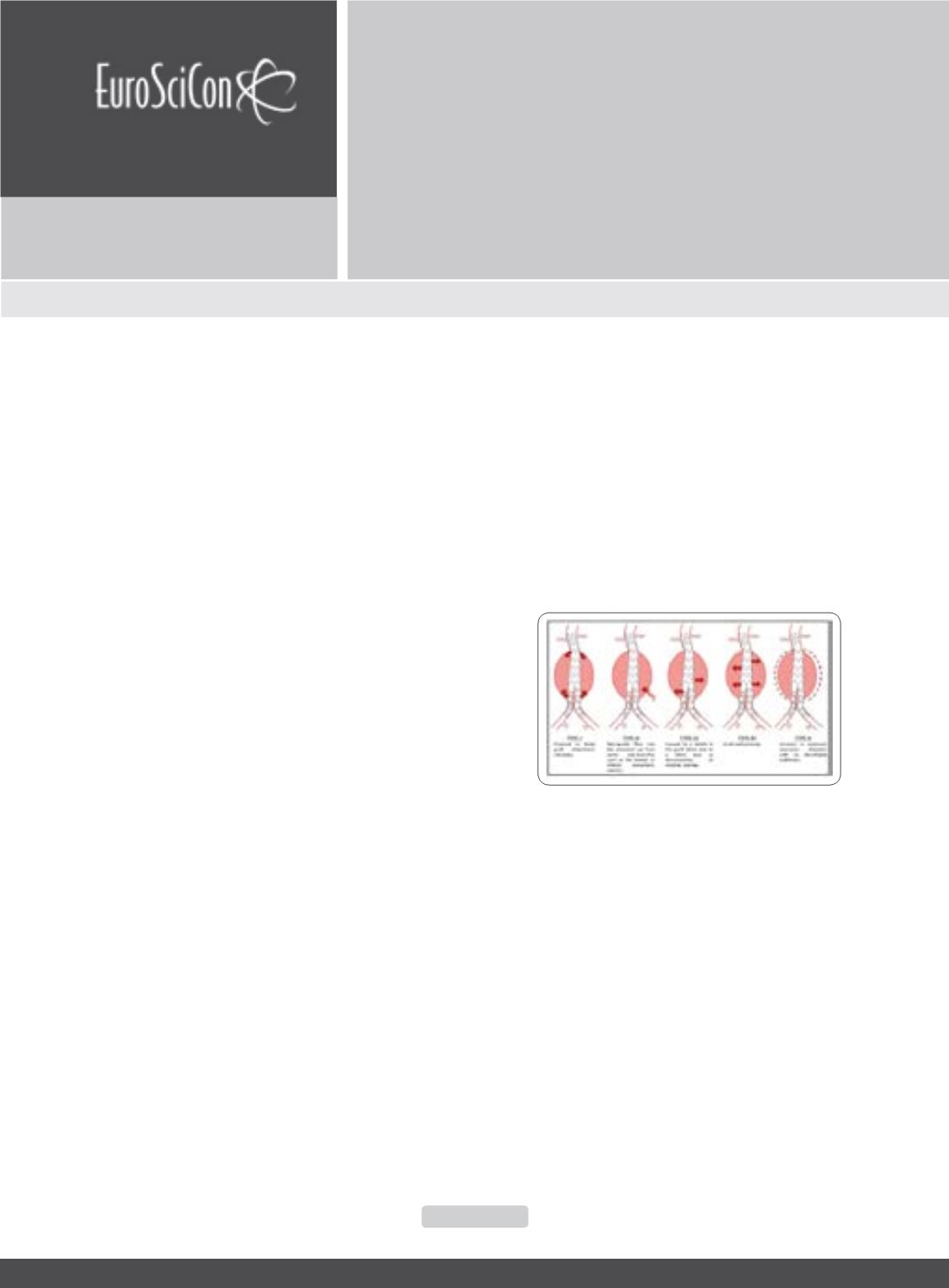
Figure 1:
Classification of Endoleaks: Endoleaks transpire due
to continued blood flow through the aneurysm site because of
incomplete graft sealing, or back-filling from supplementary
small vessels originating from the aneurysm wall. This peri-
graft blood flow may lead to saccular enlargement and rupture.