













 2 / 46
2 / 46

Pain Management 2019 & Internal Medicine 2019
International Journal of Anesthesiology & Pain Medicine
ISSN: 2471-982X
Page 39
JOINT EVENT
7
th
Edition of International Conference on
Pain Management
8
th
Edition of International Conference on
Internal Medicine &
Patient Care
&
March 25-26, 2019
Rome, Italy
Khushali Jhaveri, Int J Anesth Pain Med 2019, Volume 5
DOI: 10.21767/2471-982X-C1-006
A rare case of Intramedullary spinal ependymoma
presenting as isolated neck pain
Khushali Jhaveri
Georgetown University Washington Hospital Center, USA
A previously healthy 26 year old female presented with
initial symptom of isolated neck pain. She denied any
headache, nausea, vomiting, blurry vision, numbness,
tingling, muscle weakness or radiating pain. She denied
any fever, fatigue, joint pain, recent trauma, travel, sick
contacts or changes in weight or appetite. No risk factors
for HIV were identified.
Patient was afebrile with normal vital signs. On physical
examination, isolated neck tendernesswas notedwithout
any redness or swelling. Range of motion was preserved.
Nuchal rigidity, Kernig and Brudzinki’s sign were negative.
Neuro exam revealed 5/5motor strength in all extremities
and intact sensation in all dermatomes. Normal reflexes
were noted. Chest, cardiovascular, abdominal and
extremities examination were unremarkable.
Initial laboratory examination including CBC with
differential, inflammatory markers, renal and liver
function were within normal limits. X-ray was done
and was unremarkable. A trial of muscle relaxants
was given. On non-resolution of symptoms, An MRI
of the cervical spine was offered which revealed a
heterogenous intramedullary lesion raising suspicion for
an intramedullary neoplastic lesion. Screening of entire
CNS was otherwise unremarkable.
To establish a specific diagnosis, patient underwent
a posterior cervical laminectomy for tumor resection.
Gross-total resection was not achieved due to drop
in somatosensory potentials during intraoperative
monitoring. Histopathological examination showed WHO
grade 2 ependymoma.
Patient had no significant motor neurological impairment
after surgery. However, significant sensory and
proprioceptive loss was observed due to posterior spinal
approach. She remains progression free at 1 year with
MRI with stable residual tumor.
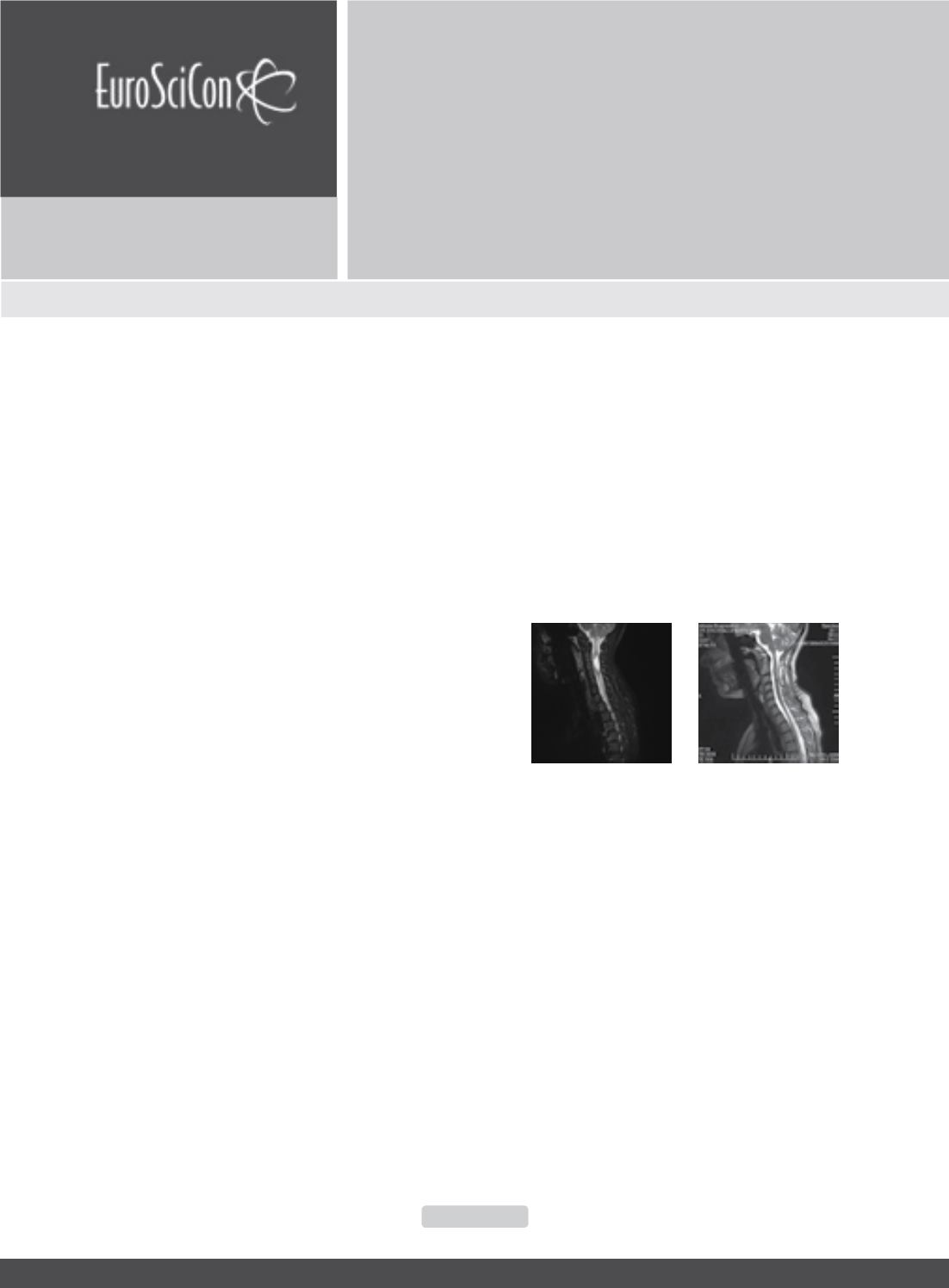
Figure 1:
Heterogenous intramedullary lesion having enhanc-
ing solid-cystic component frommid body of C2 to upper body
of C4 vertebral levelsmeasuring 36mmX 15mmX 13mmwith
solid enhancing component of the lesion measuring 13mm X
11mm X 13mm(CC X AP X Transverse). Perilesional edema
and two tiny hemorrhagic foci, one at the cranial and one at the
caudal aspect of the lesion.
Figure 2 :
Residual tumor of 13mmX 11mmX 7mm (CC X AP
X Transverse) with resolution of cystic component. Interverte-
bral disc appeared unremarkable with vertebral bodies being
normal in size, shape, alignment and signal intensity.
Biography
Khushali Jhaveri is doing her Internal medicine Residency from
Georgetown University. She has done around 5 abstract/post-
er presentations in reputed international conferences
khushali.jhaveri@gmail.com