ISSN : 2471-8041
Medical Case Reports
Can almost-fully gangrenous midgut, completely survive?
International Conference on Physicians, Surgeons and Case Reports
November 19-20, 2018 Paris, France
Hamid Qoura, Abdulrasheed, Ahmed Aboshosha, Moenes A L Karim and Adil Mohamed
Nizwa Hospital, Oman
ScientificTracks Abstracts: Med Case Rep
DOI: 10.21767/2471-8041-C2-005
Abstract
A case of duplication cyst presented with almost fully gangrenous midgut in a neoborn. Gastrointestinal (GI) duplications are rare congenital malformations that may vary greatly in presentation, size, location, and symptoms. GI duplications may present as solid or cystic swelling, intussusception, perforation, or GI bleeding or very rare volvulus. In our case, a neoborn presented with intestinal obstruction and investigations pointed to intestinal obstruction due to duplication cyst. Laparotomy findings showed near total midgut volvulus causing strangulation with subsequent almost fully gangrenous bowel and a large duplication cyst at the proximal jejunum. Bowel colour did not improve after about one hour of de-rotation, warm fomentation and increased O2 supply. Depending on specific criteria, we resected only the duplication cyst and we did primary intestinal anastomosis. Abdomen was closed without a drain. We put specific parameters for post-operative observation and explained to parents that we will observe and may need relaparotomy after 48- 72 hours if there is deterioration of the vitals, deranged investigation parameters and/or worsening of general condition of the baby. Baby improved and bowel survived. Barium meal follows through after one year showed normal bowel distribution and peristalsis. This is the first case report in such pathology and may change the view of management of near fully gangrenous bowel not improving with intraoperative manipulation.
Discussion: We reviewed articles on duplication cyst and its complications, Also articles in midbowel gangrene and its management and the prognosis.
Conclusion: The criteria which were used in taking the decision to close the abdominal cavity, were the first time to be used in such highly compromised, ischemic bowel: arterial pulsation of the mesenteric arteries started to be felt; the colour still dark but spots of pinkish discolouration appeared (Figure1); little venous blood ooze, at the cut edges of the intestine, no need to wait for arterial bleeding; weak or no clear peristalsis; the bowel doesn’t look mummified or 100% dead on benching it. The use of post-operative monitoring method is commonly used in critical patients. Full counselling to the parents in all points is a must. The success of this case deserves applying these criteria in cases of almost fully gangrenous bowel especially in such cases because removal of the affected midgut bowel will end in short bowel syndrome with its known morbidity and mortality. Also keeping the bowel in the abdominal cavity without full closure will add morbidity and will prevent the full natural environment of the bowel for survival, which I think was the main factor for the bowel to regain its viability in our case. We need more cases to prove these criteria in such conditions.
Biography
Dr Hamid Qoura, is Graduated from Kasr El-Aini medical school, (Faculty of medicine Cairo University) 1983. Finished his Master degree from the same college. Had MRCS from Ireland and FEBPS from Glasgow. Had a diploma in laparoscopic surgery from Strasbourg, France. He is working at present as a consultant and HOD of Pediatric Surgery in Nizwa Hospital, Oman. He published more than 10 papers in reputed Journals. Has special interest in laparoscopic surgery. He is the first one did real single port laparoscopic umbilical hernia, epigastric hernia and divarication of recti repair. And can do throus the same port inguinal hernias of the same patient.
E-mail: qora21@gmail.com
Google Scholar citation report
Citations : 241
Medical Case Reports received 241 citations as per Google Scholar report
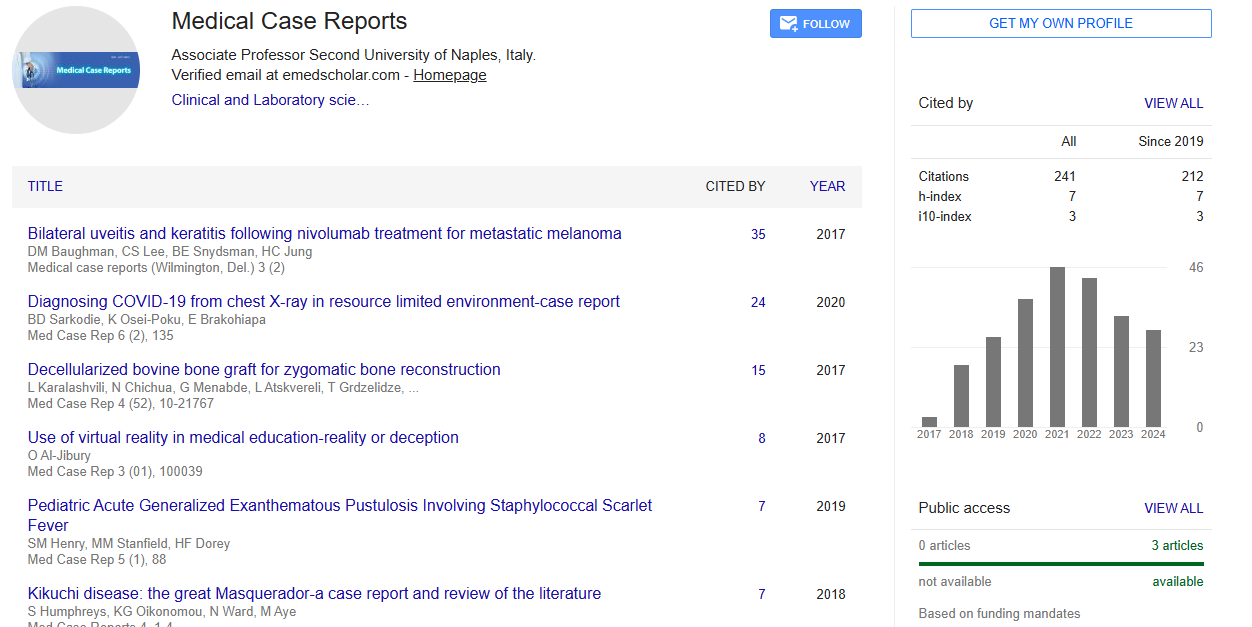
Medical Case Reports peer review process verified at publons
Abstracted/Indexed in
- Google Scholar
- China National Knowledge Infrastructure (CNKI)
- Cosmos IF
- Directory of Research Journal Indexing (DRJI)
- WorldCat
- Publons
- Secret Search Engine Labs
- Euro Pub
Open Access Journals
- Aquaculture & Veterinary Science
- Chemistry & Chemical Sciences
- Clinical Sciences
- Engineering
- General Science
- Genetics & Molecular Biology
- Health Care & Nursing
- Immunology & Microbiology
- Materials Science
- Mathematics & Physics
- Medical Sciences
- Neurology & Psychiatry
- Oncology & Cancer Science
- Pharmaceutical Sciences