Is Mycobacterium africanum Constitute a Public Health Problem in Douala: The Most Cosmopolite Town of Cameroon
Onana Ariane Tatiana1, Koro Koro Francioli1,2*, Mokam Fotso Blanche3, Ateugieu Guemechieu Romaric1, Tchamba Magloire4, Somo Moyou Roger4, Ngono Ngane Rosalie Annie1 and Etoa François-Xavier5
1Department of Biochemistry, Faculty of Sciences, University of Douala, Cameroon
2Mycobacteriology Service, Reference Laboratory of NTP, Centre Pasteur of Cameroon, Cameroon
3High Institute of Health of Banganté, University of Montagnes, Cameroon
4Veterinary Department, University of Montagne, Cameroon
5Department of Microbiology, Faculty of Sciences, University of Yaoundé I, Cameroon
- *Corresponding Author:
- Koro Koro Francioli
Department of Biochemistry
Faculty of Sciences, University of Douala
Cameroon and Mycobacteriology Service
Reference Laboratory of NTP
Centre Pasteur of Cameroon, Cameroon
Tel: 2372231015
E-mail: korokorogozion@yahoo.fr
Received Date: February 09, 2018; Accepted Date: March 16, 2018; Published Date: March 22, 2018
Citation: Onana AT, Koro KF, Mokam FB, Ateugieu GR, Tchamba M, et al. (2018) Is Mycobacterium africanum Constitute a Public Health Problem in Douala: The Most Cosmopolite Town of Cameroon. J Mol Microbiol. Vol.2 No.1:4
Abstract
Background: Mycobacterium africanum continue to cause many cases of tuberculosis in Central West African countries, while in Cameroon, it’s decreasing and M. tuberculosis mostly represented by a “Cameroon family” is increasing. Actually these observations were based in studies done in few regions of Cameroon. Materials and findings: A cross section study was therefore done in Douala one of the most cosmopolite town of Cameroon. 707 patients consulting for tuberculosis were examined and sputum was collected. Acid-fast bacilli (AFB) were detected on Ziehl-Neelsen stained impression smear and culture was made in Löwenstein-Jensen and in Löwenstein-Jensen media supplemented with 0.4% of pyruvate. Isolated strains were typed using spoligotyping and MIRU-VNTR typing. Among the 707 sputa collected, 371 were positive in culture. The molecular typing revealed that 97.3% (354/364) of cases were due to M. tuberculosis mostly represented by ST61 clad and 2.74% (10/364) to M. africanum. No M. bovis was present. Conclusion: This trend shows a high proportion of Cameroon family and evidence the low contribution of M. africanum on pulmonary TB compared to others region of Cameroon.
Keywords
Genetic structure; Mycobacterium tuberculosis; Mycobacterium africanum; spoligotyping, Douala
Introduction
Tuberculosis is still a public health problem in Cameroon with an estimated incidence of 220 cases per 100,000 in 2014 [1]. Moreover, the TB-HIV co-infection remains high representing 34% of case [1].
It is now known that molecular typing of M. tuberculosis complex (MTBC) strains can greatly help our understanding of population structure and strains circulation of the MTBC and may help improve TB control [2] and help the understanding of the population dynamic of strains of this evil disease.
In Cameroon, the use of spoligotyping in sparse studies showed a striking regression of M. africanum as etiologic agent of pulmonary tuberculosis [2-6] while this sub-specie remains endemic in others West and Central African regions countries among which Nigeria and Chad neighbouring Cameroon [7,8]. These studies also showed the predominance of a group of M. tuberculosis strains named “Cameroon family” [2-6]. This situation remains intriguing for the comprehension of molecular epidemiology of tuberculosis. But all these results are only localized in very few regions of Cameroon. To date, more than five regions over the ten that count Cameroon have unavailable data on tuberculosis genetic structure and strains circulating. Among these is the Littoral region which includes Douala, which is the most populated and cosmopolite town in Cameroon with an approximate population of 3 million and which presents a high TB transmission rate [9]. Furthermore, Douala provides 35% of TB-HIV co-infected patient which represent approximately one third of confection in the whole country [1].
In this study we aimed to establish the genetic structure of MTBC strains circulating in one of the most cosmopolite city in Cameroon in comparison to those who were previously studied, and their association to coinfection TB-HIV.
Materials and Methods
Ethical Considerations
This study obtained institutional permission N° 2015/115/UDM/ PR/CAB/CIE from the Regional Ethics Committee of University of Montagnes in Banganté-Cameroon, the authorization of the regional delegate of Health in the Littoral region N° 571/L/ MINSANTE/DRSPL/BCASS. The patients were included in the study, after understanding the aims of the research and having signed an informed consent.
Study design
We conducted a cross section study in Douala during six months (March to September 2015) 707 consecutives patients coming for TB examination were screened and their sputum were collected, in four major diagnostic and treatment centers (DTC) included in our study. These DTCs were chosen because of the high affluence and the heterogeneity of patients they received. They were from different districts (Regional administrative subdivisions) which are Nylon, Barcelon, Cité des Palmiers and Bonassama, Sociodemographic characteristics (Age, Sex, occupation, dwelling place) and other related TB risk factors information (TB history) questionnaire were administered to each patient during clinical interview by Medical staff and us, Two Sputum were collected; Microscopic exam was done using the Ziehl-Neelsen staining. Only sputa of newly diagnostic patient with pulmonary tuberculosis with positive microscopy (TPM+) and pulmonary tuberculosis with negative microscopy (TPM-) patients with highly TB clinic characteristic suspicion were finally retained for culture and molecular analysis. Sputa were collected and transported to the Laboratory on Tuberculosis Research (LTR, one of the research laboratory of University of Yaoundé open by the EDCTP fund that is situated in Yaoundé the political and administrative capital town of Cameroon) into a cetylpyridinium chloride (CPC) (1%) according to the recommendation of International Union against Tuberculosis and Lung Diseases (IUATLD).
HIV Diagnosis: We use a rapid HIV diagnosis test (DetermineTMHIV-1/2 SET) to identify HIV in TB patients. When the test was positive, confirmation was obtained by the OraQuick@ADVANCE Rapid HIV-1/2 Test (OraQuick – OraSure Technologies Inc, Bethlehem, PA, USA). If this was positive, the patient was considered to be HIV positive.
Culture: The sputa convey to the LTR were washed three times with sterile distilled water through centrifugation during 20 min. The supernatant was thrown each time. Three Lowenstein- Jensen (L- J) slants, two containing 0.75% glycerol without pyruvate and one containing 0.4% pyruvate, were inoculated with approximately 0.1 to 0.3ml of the suspended sediment and incubated at 37˚C Cultures were considered negative when no colonies were seen after eight weeks of incubation. Isolates were harvested and DNA extraction was performed as described in our previous report [6].
Molecular Analysis
Spoligotyping: Spoligotyping was performed as described by Kamerbeek et al. [10].
MIRU/VNTR typing: A MIRU/VNTR system locus used was the 5 ETR (Extremely Tandem Repeat) set A, B, C, D and E. These were individually amplified and analyzed as previously described [11].
Data analysis: Statistical analysis was performed through the Startview software version 5.0. The associations between variables (genetics profiles and phenotypic characters) were assessed by using the exact test of Fisher. The Hunter-Gaston discriminatory index (HGDI) was used to estimate the discriminatory power of MIRU-VNTR and spoligotyping.
Results
Sociodemographic data
For the 707 examined patients, 330 were positive in Ziehl- Nelseen coloration while 364 of them were positive in culture. Their age varies from 15 and above, and the most represented population age’s ranges were from the most active population (25 to 44 years). The main activity of patients was trade marker, students, and housewife. One hundred fifty-two were Women and two hundred twelve are men; this corresponded to a sex ratio (male/female) of 1.40.
TB-HIV co-infection
98% (693/707) of patients consented for HIV test. All the positive cases were TB positive. This corresponds to a TB-HIV confection rate of 16.1% (112/693) with 75% (84/112) of women versus 25% (28/112) of men infected.
Identification and genotyping of MTBC strains
Spoligotyping: Three hundred and sixty-four isolates were typed using Spoligotyping. From this, 2.74% (10/364) was from M. africanum and 97.3% (354/364) were from M. tuberculosis specie (Table 1). No M. bovis was identified.
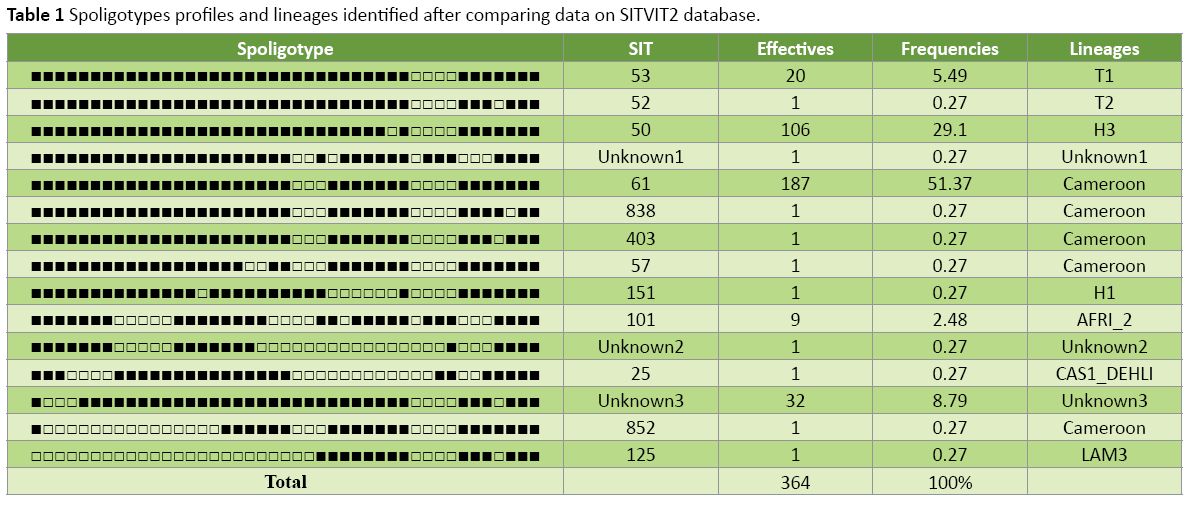
Fifteen spoligotypes patterns were identified. Among these, twelves were described in SITVITWEB database and represent 90% (330/364) of total strains. The others spoligotypes patterns were not yet described in SITVITWEB database and were call “Unknown”. Among these unknown profiles, one was clustered to 32 strains.
To the 354 M. tuberculosis strains identified, 191 (53.93%) belonged to Cameroon family which was mostly represented by SIT 61 (97.39%). Other shared-type of Cameroon family were the SIT 838, SIT 852 SIT 403 and SIT 57. All these SIT had only one strain. The others described families of M. tuberculosis families were Haarlem (29.37%) represented by lineage H3 (SIT 50; 106 strains) and H1 (SIT151; 01 strain); the ubiquitous T family (5.76%) represented by lineage T1 (SIT53; 20 strains) and T2 (SIT 52; 01 strain).
The M. africanum pattern identified (2.74%) was mainly organized in MAF1 represented by AFRI_2 lineage (SIT101; 09 strains) (Table 1). No M. africunum was identifying among the coinfected HIV patient.
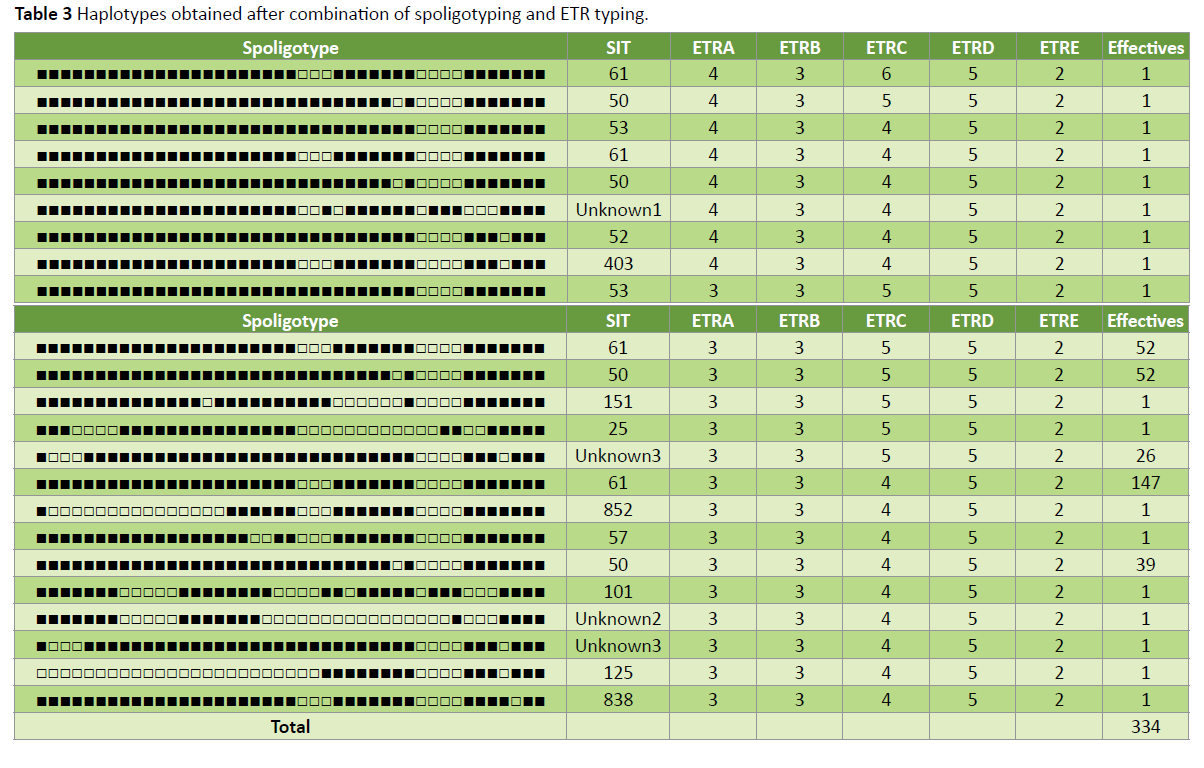
MIRU-VNTR: Three hundred and thirty-four strains have been analyzed using the five ETR systems. From these only five haplotypes were identified corresponding to a genetic diversity of 0.18.
Two loci were found polymorphic: ETR A (two alleles) and ETR C (three alleles) (Table 2). The other was monomorphic.

Spoligotyping and MIRU-VNTR association: ETR typing and spoligotyping were combined to analyse the genetic diversity of MTBC isolates. The genetic diversity observed was 0.17. This remains extremely low. Despite this, 23 profiles were identified different from the fifteen and five obtained respectively for Spoligotyping and ETR typing alone. The SIT61, SIT 50, SIT 53 profiles were divided respectively into four, four and two profiles when associated to the ETR typing (Table 3).
Discussion
Tuberculosis remains a public Health preoccupation in Cameroon since most registered cases concern active population [2-6] our study is confirming this trend. More over TB-HIV co-infection rate remains high (16.1%) in our study, this value is nevertheless less compare to the value reported in Douala [1] and in Adamaoua [6]. The reasons are unknown.
Sparse molecular epidemiology studies done in certain region in Cameroon have shown the very weak contribution of M. africanum to pulmonary tuberculosis and the predominance of M. tuberculosis represented by Cameroon family. We have make for the first time a study in a more populated and cosmopolite town in Cameroon in order to verify this genetic structure trend and to gain more information about the genetic structure of MTBC strains in Douala. Our result shows a very weak contribution of M. africanum in pulmonary tuberculosis in Douala. This result is similar to that described by Koro Koro and collaborators in Adamaoua [6]. But remain lesser than those describes in others central West African countries [8,12-15]. We also observed that all M. africanum strain isolated in our study were from HIV negative patients. This observation raises once again the question why M. africanum is very weak in Cameroon while in most Central West African countries it remains high? This is very intriguing but we noticed that all M. africanum in Cameroon is not isolated in HIV positive person. Moreover, we think that the Cameroonian M. africanum species have different feature as those of the others countries (personal Data). We also think that strains’ belonging to these species has different selective habits including virulence and pathogenesis or that systematical introduction of vaccination in new born baby in Cameroon may have selected some species or genotypes.
All the M. africanum isolated were MAF1 mainly represented by AFRI-2 lineage characterised by it clad SIT 101 clustered to 9 strains. The predominance of AFRI-2 in Cameroon has been also described in all the studies done in Cameroon [2-6] particularly the SIT101 which have shown to be also clustered even in West [5] and in Adamaoua region [6]. This result might suggest that the strain of this clade might be actively implicated in TB transmission in Cameroon.
M. tuberculosis has been proved to be prevalent among MTBC strains isolated in Cameroon. Our study confirms this trend which is similar to the proportion obtained in the Center region (97%) [3], although it shows a higher proportion compare to 96% obtained in Adamaoua [6] and West region [5]. More over our study shows a very high proportion of Cameroon family (54%) and SIT61 clad (51%) in Douala. This result is higher than those observed in West region (48% and 29% respectively) [5] and closer to those obtained in Adamaoua region (66% and 53% respectively) [6] and in the Center region (51.01% and 42.95%) [3].
Our study shows a very less genetic diversity in M. tuberculosis species and in Cameroon Family or in SIT61 Clad even by the use of spoligotyping and ETR typing alone or combined. This result might traduce the active TB transmission even among Douala citizen. This result confirms the study done in 2014 in Douala and that shows evidence of clustering of pulmonary tuberculosis cases in Douala [9]. But when considering the homoplasy phenomenon due to spoligotyping and the system of five ETR used in this study we think that this clustered even need to be verify by the used of more consistent number of MIRU-VNTR for typing of this MTBC strains.
Conclusion
The aim of this work was to evaluate the impact of M. africanum as a causative agent of tuberculosis in Douala, one of the most cosmopolite towns in Cameroon, since this specie had showed a genuine regression in others regions of Cameroon. This work revealed a weak contribution of M. africanum in pulmonary tuberculosis with a value lesser than those described in others regions of Cameroon. However, it shows an increase of M. tuberculosis represented by a Cameroon family clad SIT61. The reasons of this trend need to be investigated in other to understand the circulation and adaptation of MTBC strain in different regions.
Acknowledgments
We acknowledge the support of the Centre Pasteur of Cameroon and the Laboratory of Tuberculosis Research in the realization of this research.
Funding
This project did not receive external grant funding. The cost for genotyping was covered by the internal fund of University of Douala.
References
- Trébucq A, Koura G (2014) Rapport N°20 Union InternationaleContre la Tuberculose et les Maladies Respiratoires, PNLT Report 2014.
- Niobe-Eyangoh SN, Kuaban C, Sorlin P, Cunin P, Thonnon J,et al., (2003) Genetic biodiversity of Mycobacterium tuberculosis Complex Strains from Patients with Pulmonary Tuberculosis in Cameroon. J Clin Microbiol 41: 2547-2553.
- Kamgue SL, Mouafo TE, Kuaban C, Assam Assam JP, Tedom JC, et al., (2013) Estimates of Genetic Variability of Mycobacterium tuberculosis Complex and Its Association with Drug Resistance in Cameroon. AdvInfect Dis 3: 55-59.
- Assam Assam JP, PenlapBeng V, Cho-Ngwa F, Toukam M, Ane-Anyangwe IN et al., (2013) Mycobacterium tuberculosis is the causative agent of tuberculosis in the southern ecological zones of Cameroon, as shown by genetic analysis. BMC Infect Dis 13:431.
- KoroKoro F, Kamdem SY, Fotso P F, Noeske J, Gutierrez C et al., (2013) Population Dynamics of Tuberculous Bacilli in Cameroon as Assessed by Spoligotyping. J Clin Microbiol 51: 299-302.
- KoroKoro F, Um Boock A, Kaiyven AL,Noeske J, Gutierrez C, et al., (2016) Genetic Structure and Drug Susceptibility Patterns of Mycobacterium tuberculosis Complex Strains Responsible of Human Pulmonary Tuberculosis in the Major Rearing Region in Cameroon. Bio Med Res Int 2016: 2904832
- Diguimbaye C, Hilty M, Ngandolo R, Mahamat HH, Pfyffer GE, et al., (2006) Molecular characterization and drug resistance testing of Mycobacterium tuberculosis isolates from Chad. Journal of Clinical Microbiology. 44:1575-1577.
- Thumamo BP, Asuquo AE, Abia-Bassey LN, Lawson L, Hill V, et al., (2011) Molecular epidemiology and genetic diversity of mycobacterium tuberculosis complex in the cross river state, Nigeria. Infect Genet Evol 12: 671-677.
- Nana Y, Noeske J, Dambach P, Bowong S, Fono LA, et al., (2014) Spatial analysis of tuberculosis in Douala, Cameroon: clustering and links with socio-economic status. IntJ Tuber Lung Dis 18:292-297.
- Kamerbeek J, Schouls L, Kolk A, Van Agterveld M, Van Soolingen D, et al., (1997) Simultaneous detection and strain differentiation of Mycobacterium tuberculosis for diagnosis and epidemiology. J Clin Microbiol 35:907-914.
- Supply P, Mazars E, Lesjean S, Vincent V, Gicquel B et al., (2000) Variable human minisatellite-like regions in the Mycobacterium tuberculosis genome. Mole Microbiol 36: 762-771.
- De Jong B, Antonio M, Gagneux S (2010) Mycobacterium africanum-Review of an Important Cause of Human Tuberculosis in West Africa. PLoSNegl Trop Dis 4: 744.
- Yeboah-Manu D, Asante-Poku A, Bodmer T, Stucki D, Koram K, et al., (2011) Genotypic Diversity and Drug Susceptibility Patterns among M. tuberculosis Complex Isolates from South-Western Ghana. PLoS ONE 6: 21906.
- Gomgnimbou MK, Refrégier G, Diagbouga SP, Adama S, Kaboré A, et al., (2012) Spoligotyping of Mycobacterium africanum, Burkina Faso. Emerg Infect Dis 18: 117-119.
- Lawson L, Zhang J, Gomgnimbou MK, Abdurrahman ST, Moullec SL, et al., (2012) A Molecular Epidemiological and Genetic Diversity Study of Tuberculosis in Ibadan, Nnewi and Abuja, Nigeria. PLoS ONE 7: 38409.

Open Access Journals
- Aquaculture & Veterinary Science
- Chemistry & Chemical Sciences
- Clinical Sciences
- Engineering
- General Science
- Genetics & Molecular Biology
- Health Care & Nursing
- Immunology & Microbiology
- Materials Science
- Mathematics & Physics
- Medical Sciences
- Neurology & Psychiatry
- Oncology & Cancer Science
- Pharmaceutical Sciences