Evolution of Gait Asymmetry during Body-Weight Supported Treadmill Therapy after Common Orthopedic Surgeries: A Case Series Study
Miloslav Kubicek1 and Tomas Brozek1,2*
1Rehabilitation Center in Slapy, Slapy nad Vltavou, Czech Republic
2Department of Psychology, Charles University, Prague, Czech Republic
- *Corresponding Author:
- Tomas Brozek
Department of Psychology,
Charles University, Prague,
Czech Republic,
E-mail: tomasbrozek@centrum.cz
Received date: November 27, 2023, Manuscript No. IPGSR-23-18161; Editor assigned date: November 30, 2023, PreQC No. IPGSR-23-18161(PQ); Reviewed date: December 14, 2023, QC No. IPGSR-23-18161; Revised date: December 21, 2023, Manuscript No. IPGSR-23-18161 (R); Published date: December 28, 2023, DOI: 10.36648/ipgsr.7.2.6290
Citation: Kubicek M, Brozek T (2023) Evolution of Gait Asymmetry during Body-Weight Supported Treadmill Therapy after Common Orthopedic Surgeries: A Case Series Study. Gen Surg Rep Vol.7 No.2: 6290.
Abstract
Background: Patients recovering from surgery of the locomotor system as a result of compensation to avoid pain in the impaired segment exhibit signs of gait asymmetry up to 2 years after the procedure. An early and properly designed gait retraining protocol is key in restoring the symmetry gait pattern and returning to daily activities.
Methods: Four patients after common orthopedic surgery (total hip arthroplasty, total knee arthroplasty, anterior cruciate ligament reconstruction and tibial fracture allowed by fasciotomy) completed 6 BWSTT sessions, during which gait parameters for the affected and unaffected limb were recorded, followed by conventional rehabilitation. The evolution of the symmetry index for the parameters stance time, step length, step time, swing time and weight-bearing proportion was evaluated.
Results: An improvement in gait asymmetry was reported during the study course in all participating patients. A patient recovering from a tibial fracture complicated by compartment syndrome with the need for fasciotomy saw an improvement in all measured parameters except for swing time. On the contrary, the patient after ACL reconstruction experienced the greatest progress an almost complete symmetry restoration was observed in most gait parameters during only 6 sessions.
Conclusion: The results of the present case series study indicate that BWSTT therapy can lead to improvement and almost complete restoration of various gait parameters symmetry in patients after common lower limb surgeries.
Keywords
R-Force; Antigravity treadmill; Total knee arthroplasty; Total hip arthroplasty; Tibial fracture; Anterior cruciate ligament reconstruction; Symmetry index; Gait parameters
Introduction
The symmetry and coordination of human gait have a proven impact on walking velocity and energy expenditures and are thus an indispensable part of everyday life [1]. Impaired muscle activation, muscle weakness, pain and joint motion limitation are potential sources of gait asymmetry in patients recovering from serious injuries and lower limb surgeries [2]. Typical conditions are represented by Anterior Cruciate Ligament (ACL) surgery, Total Hip Arthroplasty (THA), Total Knee Arthroplasty (TKA), osteoarthritis, amputation of the lower limb, but also other postoperative and post-traumatic conditions of the lower extremities. Asymmetrical gait deviations arising as a result of patient limitations, such as compensation to avoid pain, can lead to an uneven load distribution and subsequently escalate into a loss of bone mineral density in the under loaded limb, the development of osteoarthritis of the contralateral limb, low back pain and a condition requiring the replacement of any joints on the contralateral limb [3].
The estimated annual incidence of TKA, THA, ACL reconstruction surgery and tibial shaft fracture in the USA is around 238, 156, 29 and 17 patients per 100,000 population, respectively [4-6]. While ACL reconstruction and tibial shaft surgery are mainly provided to the age group under 40 years, hip and knee arthroplasty is predominantly performed on patients from the older age group above 60 years [6-8]. The worldwide population aging leads to an increase in the number of patients requiring such surgical intervention and thus creates pressure for the simultaneous improvement and acceleration of postoperative rehabilitation. Postoperative physiotherapy and gait retraining are, in the case of the above-mentioned conditions, an essential part of postoperative care, enabling patients an early return to independence in daily activities. Insufficient or inappropriate post-operative rehabilitation can lead to re-injury due to overloading of the impaired segment, but also to the preservation of gait asymmetry and related musculoskeletal conditions [3]. It has been proven that in patients after ACL reconstruction, a certain form of kinematic and kinetic asymmetry persists for up to two years after surgery. Due to the lower average age of these patients and the high percentage of athletes, it can be assumed that they are interested in an early return to sports activities. The combination of asymmetric loading of the lower limbs and sports performance leads to an increased risk of second ACL injury. In patients with multi-planar biomechanical asymmetries, this risk was evaluated as three times greater than in patients without gait asymmetry [9].
A suitable manually undemanding form of gait retraining with a proven positive effect on gait asymmetry is offered by the advanced approach of Body-Weight Supported Treadmill Therapy (BWSTT) [10]. The BWSTT principle provides the patient with full or partial body-weight relief during exercise, which allows the patient to gradually increase the load during recovery and thus prevents the risk of straining the impaired segment. It is assumed that body-weight support also minimizes the patient's need to consciously or unconsciously compensate to avoid pain thereby creating an uneven load on the lower extremities. The integration of BWSTT in the early rehabilitation phase leads to a rapid restoration of the gait cycle and its symmetrical pattern, which eliminates the risk of creating a gait deviation and related musculoskeletal conditions. The positive effect of BWSTT on gait retraining has been clinically proven in neurological patients suffering from Parkinson's disease, cerebral palsy and recovering after stroke and spinal cord injury [11-20]. From disorders of the locomotion system, improvement was reported in patients who had undergone knee or hip arthroplasty, ACL reconstruction and lower extremity fracture [21-24]. The only published clinical trial focusing on the restoration of symmetry during the BWSTT program demonstrated a statistically significant reduction of asymmetry during only 6 sessions in patients after knee and hip arthroplasty [24]. This relatively unique research lacks mutual progress comparison for different locomotion disorders as well as knowledge about the detailed gait parameters development during individual sessions. The present study is designed as a case series study and aims at a detailed comparison of gait parameters and their symmetry indices development during the BWSTT treatment program among patients recovering from 4 common lower extremity surgeries.
Materials and Methods
The research was carried out as part of a routine treatment program in a rehabilitation center focusing on the recovery of traumatic and post-operative conditions of the locomotor system. Four patients recovering from selected lower extremity surgery TKA, THA, ACL reconstruction and tibial fracture willing to participate were recruited. Patients were selected with regard to the nature of BWSTT and its contraindications - severe cardiovascular disease, bronchial asthma, angina pectoris, disc herniation, pregnancy, epilepsy, or any conditions with increased abdominal pressure. The study was designed in accordance with the 1975 Declaration of Helsinki ethical guidelines adopted by the Convention on Human Rights and Biomedicine of the Council of Europe (1997) and by the general assembly of the World Medical Association (1997-2000) [25].
BWSTT therapy was performed using advanced technology (BTL Industries, Ltd.) during which the patient is weight supported using a positive-pressure chamber. This chamber surrounds the lower half of the patient's body as well as the treadmill itself. A tight connection is ensured by means of a zip mechanism between the patient's special shorts and the opening in the chamber. Once the patient is zipped in, calibration is started and the device is adjusted according to the operator's instructions and the patient's weight. BWSTT settings such as inclination, speed and percentage of weight support are adjusted at the beginning of each therapy to match the patient's current abilities and health status. It is assumed that during the treatment program these parameters will gradually increase according to the patient's progress. Inclination can be set within the range 0%-15%, body weight support in the range of 0%-100% and speed from 8 km/h to 25 km/h.
Each subject completed 6 BWSTT sessions combined with conventional rehabilitation. During BWSTT, gait parameters for the affected and unaffected limb were measured using pressure sensors integrated within the treadmill. The Symmetry Index (SI) for the parameters stance time, step length, step time, swing time and weight-bearing proportion was calculated based on equation [26,27]:
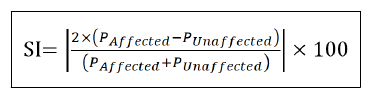
Where PAffected stands for the measured value of the respective parameter of affected limb and PUnaffected of the unaffected limb. Gait asymmetry is evaluated according to the SI value as follows:
• SI=0 full symmetry
• SI<10% acceptable between-limb difference
• SI  10% unacceptable between-limb difference
10% unacceptable between-limb difference
• SI>100 complete asymmetry
For the purpose of mutual comparison of individual indications, their parameter development during the treatment program was shown in graphs. Data processing and their visualization were performed using the Matlab program (MatLab R2010b, Mathworks, Inc., Narick, MA, USA).
Results
The therapy was accepted positively by the patients and no adverse events were reported during the trial. Details about participants can be found in Table 1.
| Surgery | Gender | Age | Affected limb |
|---|---|---|---|
| Total hip arthroplasty | W | 65 | L |
| Total knee arthroplasty | W | 61 | L |
| Anterior cruciate ligament reconstruction | M | 43 | L |
| Tibial fracture with fasciotomy | M | 38 | R |
Table 1: Patients’ demographics.
During the initial session, gait asymmetry was detected in all patients. While the largest between-limb difference across monitored gait parameters was recorded in the THA patient, the smallest asymmetry was expressed by a patient with a tibial fracture. In general, an improvement in gait asymmetry was noted during the study course in all participating patients. A patient recovering from a tibial fracture complicated by compartment syndrome with the need for fasciotomy saw an improvement in all measured parameters except for swing time. On the contrary, the patient after ACL reconstruction experienced the greatest progress an almost complete symmetry restoration was observed in most gait parameters during only 6 sessions.
Stance time
The stance time of the affected limb was significantly longer than the stance time of the unaffected limb during the first session which was confirmed by a symmetry index greater than 10 in all patients. During the last session, all participants noted an improvement in stance time symmetry by at least 50% and achieved an SI value of less than 10% meaning acceptable between-limb difference. The detailed development of stance time for individual indications throughout the treatment program is shown in Figure 1. The development of the symmetry index had a gradually decreasing trend in patients after arthroplasty, while in patients after tibial fracture and ACL reconstruction the changes were more dynamic and its evolution was accompanied by a sudden deterioration approximately halfway through the treatment program (Figure 2). Patient post ACL reconstruction experienced an almost complete restoration of stance time symmetry an improvement of more than 90% was recorded.

Figure 1: The evolution of stance time in Multiple Sclerosis (MS) for the affected and unaffected limb throughout the treatment program across respective indications.
Note: A: Total hip arthroplasty; B: Total knee arthroplasty; C: Tibial fracture; D: Knee arthroscopy; ( ): Unaffected limb; (
): Unaffected limb; (  ): Affected limb.
): Affected limb.

Figure 2: Comparison of stance time asymmetry development for individual indications.
Note: ( ): Total hip arthroplasty; (
): Total hip arthroplasty; ( ): Total knee arthroplasty; (
): Total knee arthroplasty; ( ): Tibial fracture; (
): Tibial fracture; ( ): Knee arthroscopy.
): Knee arthroscopy.
Step length
The step length of the affected limb was longer than that of the unaffected limb during almost all sessions. In the tibial fracture patient, this trend was reversed, but only during the first session (Figure 3). None of the patients showed asymmetry in terms of step length symmetry index exceeding 10%. The development of the symmetry index was accompanied by dynamic changes in almost all patients until the fifth session, after which a significant decrease occurred (Figure 4). All patients experienced an improvement of at least 30%. The TKA patient experienced the greatest step length asymmetry reduction of over 60%.

Figure 3: Bar graphs displaying the evolution of step length in cm for the affected and unaffected limb throughout the treatment program for the respective indication groups.
Note: A: Total hip arthroplasty; B: Total knee arthroplasty; C: Tibial fracture; D: Knee arthroscopy; ( ): Unaffected limb; ( ): Affected limb.

Figure 4: Curves showing the development of the step length symmetry index for patients from individual indication groups.
Note: ( ): Total hip arthroplasty; ( ): Total knee arthroplasty; ( ): Tibial fracture; ( ): Knee arthroscopy.
Step time
The step time of the affected limb was shorter than that of the unaffected limb during almost all sessions. In the tibial fracture patient, this trend was reversed, but only during the first session (Figure 5). The asymmetry value exceeded the 10% acceptance level in all patients during the first session. In the THA patient, the development of the step time symmetry index had an almost linear trend and its value during the last session was close to zero. Although the greatest asymmetry was measured in this patient during the first session, the lowest value was reported at the end of the treatment program with a total asymmetry reduction of over 90%. All other patients also experienced an improvement in step time asymmetry by at least 30% which brought them below the 10% acceptance level (Figure 6).

Figure 5: Comparison of step time between-limb difference in MS across respective indications.
Note: A: Total hip arthroplasty; B: Total knee arthroplasty; C: Tibial fracture; D: Knee arthroscopy; ( ): Unaffected limb; ( ): Affected limb.

Figure 6: Development of the step time symmetry index during the treatment course in patients with various musculoskeletal impairments.
Note: ( ): Total hip arthroplasty; ( ): Total knee arthroplasty; ( ): Tibial fracture; ( ): Knee arthroscopy.
Swing time
In the case of swing time, the trend between affected and unaffected limb is not clear. While in THA and post ACL reconstruction patients the length of swing time was more in favor of the unaffected limb, TKA and post-tibial fracture patients experienced the opposite trend (Figure 7). Three out of four patients during the first session expressed asymmetry greater than 10%, the patient after the tibial fracture started the program without significant swing time asymmetry. A mutual comparison of the symmetry index reduction between individual indications brought interesting indings. A significant decrease of more than 75% was observed in almost all patients. On the contrary, significant deterioration was noted in the patient after the tibial fracture who was the only one during the last session to show an asymmetry exceeding the SI value of 10% -all other patients reached below this level (Figure 8).

Figure 7: Bar graphs showing the evolution of swing time in MS for the affected and unaffected limb through the treatment program for the respective indications. Note: A: Total hip arthroplasty; B: Total knee arthroplasty; C: Tibial fracture; D: Knee arthroscopy; ( ): Unaffected limb; ( ): Affected limb.

Figure 8: The curve graph offering a comparison of the development of the symmetry index during individual sessions.
Note: ( ): Total hip arthroplasty; ( ): Total knee arthroplasty; ( ): Tibial fracture; ( ): Knee arthroscopy.
Weight-bearing proportion
Uneven loading of the lower extremities with a greater load on the unaffected limb with asymmetry exceeding the 10% acceptance level was observed in all patients (Figure 9). During the course of the treatment program, the asymmetry of weight distribution improved in all patients by at least 33% leading to a drop in asymmetry below the 10% level (Figure 10). The patient after ACL reconstruction experienced a complete restoration of symmetry after only 5 sessions.

Figure 9: Bar graphs showing between-limb difference in weight-bearing proportion for patients with various locomotion disorders.
Note: A: Total hip arthroplasty; B: Total knee arthroplasty; C: Tibial fracture; D: Knee arthroscopy; ( ): Unaffected limb; ( ): Affected limb.

Figure 10: Curves showing symmetry index of weightbearing proportion and its changes during individual sessions for different indications.
Note: ( ): Total hip arthroplasty; ( ): Total knee arthroplasty; ( ): Tibial fracture; ( ): Knee arthroscopy.
Discussion
From the results of the present study, due to the limited sample of subjects, it is not possible to make any complex conclusions regarding the development of gait symmetry in patients after various locomotor system operations. The main benefit of the study is the proof that BWSTT can contribute to the rapid asymmetry reduction and in some cases to almost complete symmetry restoration in the course of only 6 sessions. All parameters for which an asymmetry exceeding the 10% acceptance level was recorded during the first session reached a value of less than 10% during the SI treatment program, which leads to the assumption that BWSTT therapy enables effective gait retraining with the aim of symmetry restoration. The patient after ACL reconstruction achieved the greatest overall improvement across the symmetry indexes of individual parameters. Comparable results were also reported by the THA patient, who, together with the patient after ACL reconstruction and TKA, recorded a reduction in the asymmetry of all monitored parameters. A patient recovering from a tibial fracture complicated by compartment syndrome with the need for fasciotomy recorded an improvement in all parameters except swing time. This patient expressed the smallest degree of asymmetry before starting the treatment program and thus experienced the smallest improvement.
The length of postoperative recovery is highly individual and influenced by many factors such as gender, age, preoperative condition of the limb, type and length of surgery, postoperative rehabilitation and others [28,29]. Summarizing generally valid knowledge about the length of recovery for individual interventions can bring better insight into the results of the present case series study.
Total recovery time for patients after arthroplasty is, according to the available evidence, shorter for the hip than for the knee, lasting approximately 2-6 and 3-12 months, respectively [30]. However, the time for which patients are recommended to walk with the support of crutches is the same, approximately 6 weeks [31,32]. Comparing the recovery time with patients after ACL reconstruction may not be completely accurate, given that a large percentage of operated patients are athletes who expect a full return to sports after surgery within one year of injury. According to a recent study, the time required for discontinuing crutches is around 15 days [33]. Acute compartment syndrome requiring fasciotomy can cause delay in tibial fracture union. Clinical evidence states the average time required for full weight-bearing is 25 weeks and the minimum time for walking without crutches is 8 weeks [34,35]. The age distribution of the study participants corresponds to the average age of the patients of the respective indication, just as their results correlate with the aforementioned recovery times. Age and gender did not appear to be major factors influencing therapy outcomes. The youngest patient after the tibial fraction experienced the slowest progression due to compartment syndrome. The second youngest participant recovering after ACL reconstruction experienced the greatest reduction in asymmetry. Without knowing his background, sports activity and motivation for an early return, no further conclusions can be made. A comparable improvement was also achieved by the THA patient, who, however, expressed a greater degree of asymmetry during the first session. A TKA patient would probably need more sessions to achieve similar results, mainly due to the more complicated surgery and greater complexity of the knee joint [30].
The main limitation of the study has already been mentioned - the case series study does not allow making generally valid conclusions, these purposes require recruiting several patients for each indication. At the same time, it would be appropriate to treat half of the patients with conventional physiotherapy combined with BWSTT and the other half only with conventional physiotherapy. This control group would allow mutual comparison and evaluation of the effectiveness of standalone BWSTT.
The present study demonstrated that patients after routine lower limb surgeries can benefit from BWSTT. Its results can serve as a starting point for larger-scale research that further quantifies therapy outcomes for different musculoskeletal indications.
Conclusion
The results of the present case series study indicate that BWSTT therapy can lead to improvement and almost complete restoration of various gait parameters symmetry in patients after common lower limb surgeries. The magnitude of improvement may vary depending on the complexity of the surgical intervention and the recovery time required for the tissue to heal.
References
- Plotnik M, Wagner JM, Adusumilli G, Gottlieb A, Naismith RT (2020) Gait asymmetry and bilateral coordination of gait during a six-minute walk test in persons with multiple sclerosis. Sci Rep 10: 12382.
[Crossref], [Google Scholar], [Indexed]
- Christiansen CL, Bade MJ, Weitzenkamp DA, Stevens-Lapsley JE (2013) Factors predicting weight-bearing asymmetry 1 month after unilateral total knee arthroplasty: A cross-sectional study. Gait Posture 37: 363-367.
[Crossref], [Google Scholar], [Indexed]
- Cabral S (2018) Gait symmetry measures and their relevance to gait retraining. Handbook of Human Motion: 429-447.
[Crossref], [Google Scholar]
- Shah B (2023) Joint replacement surgery.
- Evans J, Nielson Jl (2022) Anterior cruciate ligament knee injury. Treasure Island: StatPearls Publishing.
- Larsen P, Elsoe R, Hansen SH, Graven-Nielsen T, Laessoe U, Rasmussen S (2015) Incidence and epidemiology of tibial shaft fractures. Injury 46: 746-750.
[Crossref], [Google Scholar], [Indexed]
- Leathers MP, Merz A, Wong J, Scott T, Wang JC, et al. (2015) Trends and demographics in anterior cruciate ligament reconstruction in the United States. The Journal of Knee Surgery 28: 390-394.
[Crossref], [Google Scholar], [Indexed]
- Fang M, Noiseux N, Linson E, Cram P (2015) The effect of advancing age on total joint replacement outcomes. Geriatr Orthop Surg Rehabil 6: 173-179.
[Crossref], [Google Scholar], [Indexed]
- Sharafoddin-Shirazi F, Letafatkar A, Hogg J, Saatchian V (2020) Biomechanical asymmetries persist after ACL reconstruction: Results of a 2-year study. J Exp Orthop 7:1-86.
[Crossref], [Google Scholar], [Indexed]
- Kubícek M, Brozek T (2023) The effect of body-weight supported treadmill therapy program on the gait asymmetry in patients after lower limb arthroplasty. Adv Tech Biol Med 11: 415.
[Crossref]
- Covarrubias-Escudero F, Rivera-Lillo G, Torres-Castro R, Varas-Díaz G (2019) Effects of body weight-support treadmill training on postural sway and gait independence in patients with chronic spinal cord injury. J Spinal Cord Med 42: 57-64.
[Crossref], [Google Scholar], [Indexed]
- Plummer P, Behrman AL, Duncan PW, Spigel P, Saracino D, et al. (2007) Effects of stroke severity and training duration on locomotor recovery after stroke: A pilot study. Neurorehabil Neural Repair 21: 137-151.
[Crossref], [Google Scholar], [Indexed]
- Duncan PW, Sullivan KJ, Behrman AL, Azen SP, Nadeau SE, et al. (2011) Body weight supported treadmill rehabilitation after stroke. N Engl J Med 364: 2026-2036.
[Crossref], [Google Scholar], [Indexed]
- Lura DJ, Venglar MC, van Duijn AJ, Csavina KR (2019) Body weight supported treadmill vs. overground gait training for acute stroke gait rehabilitation. Int J Rehabil Res 42: 270-274.
[Crossref], [Google Scholar], [Indexed]
- Atan T, Taskiran OO, Tokcaer AB, Karatas GK, Caliskan AK, et al. (2019) Effects of different percentages of body weight supported treadmill training in Parkinson‘s disease: A double-blind randomized controlled trial. Turk J Med Sci 49: 999-1007.
[Crossref], [Google Scholar], [Indexed]
- Combs SA, Dugan EL, Ozimek EN, Curtis AB (2013) Bilateral coordination and gait symmetry after body-weight supported treadmill training for persons with chronic stroke. Clin Biomech 28: 448-453.
[Crossref], [Google Scholar], [Indexed]
- Lotfian M, Dadashi F, Rafieenazari Z, Shahroki A, Rasteh M, et al. (2019) The effects of anti-gravity treadmill training on gait characteristics in children with cerebral palsy. Annu Int Conf IEEE Eng Med Biol Soc: 5256-5259.
[Crossref], [Google Scholar], [Indexed]
- Miller EW, Quinn ME, Seddon PG (2002) Body weight support treadmill and over ground ambulation training for two patients with chronic disability secondary to stroke. Phys Ther 82: 53-61.
[Crossref], [Google Scholar], [Indexed]
- Prunerová A, Vinarov E (2023) Increase in metabolic rate and related parameters during an antigravity treadmill exercise program in neurological patients. J Neurodegenero Dis Disord 6: 4.
[Crossref]
- McCain KJ, Pollo FE, Baum BS, Coleman SC, Baker S, et al. (2008) Locomotor treadmill training with partial body-weight support before over ground gait in adults with acute stroke: A pilot study. Arch Phys Med Rehabil 89: 684-691.
[Crossref], [Google Scholar], [Indexed]
- Palke L, Schneider S, Karich B, Mende M, Josten C, et al. (2022) Anti-gravity treadmill rehabilitation improves gait and muscle atrophy in patients with surgically treated ankle and tibial plateau fractures after one year: A randomised clinical trial. Clin Rehabil 36: 87-98.
[Crossref], [Google Scholar], [Indexed]
- Hesse S, Werner C, Seibel H, von-Frankenberg S, Kappel EM, et al. (2003) Treadmill training with partial body-weight support after total hip arthroplasty: A randomized controlled trial. Arch Phys Med Rehabil 84: 1767-1773.
[Crossref], [Google Scholar], [Indexed]
- Webber SC, Horvey KJ, Yurach-Pikaluk MT, Butcher SJ (2014) Cardiovascular responses in older adults with total knee arthroplasty at rest and with exercise on a positive pressure treadmill. Eur J Appl Physiol 114: 653-662.
[Crossref], [Google Scholar], [Indexed]
- Savarino D, Prunerova A (2023) Comparison of therapeutic progression using anti-gravity treadmill for different postoperative and post injury conditions. J Clin Exp Orthopr 9: 401.
[Crossref]
- Council of Europe (1997) Convention for protection of human rights and dignity of the human being with regard to the application of biology and biomedicine: Convention on human rights and biomedicine. Kennedy Inst Ethics J 7: 277-290.
[Crossref], [Google Scholar], [Indexed]
- Wu J, Wu B (2015) The novel quantitative technique for assessment of gait symmetry using advanced statistical learning algorithm. BioMed Res Int 528971.
[Crossref], [Google Scholar], [Indexed]
- Queen R, Dickerson L, Ranganathan S, Schmitt D (2020) A novel method for measuring asymmetry in kinematic and kinetic variables: The normalized symmetry index. J Biomech 99: 109531.
[Crossref], [Google Scholar], [Indexed]
- Zhang S, Huang Q, Xie J, Xu B, Cao G, et al. (2018) Factors influencing postoperative length of stay in an enhanced recovery after surgery program for primary total knee arthroplasty. J Orthop Surg Res 13: 29.
[Crossref], [Google Scholar], [Indexed]
- Rahman A, Mahdy N, Kamaly A (2017) Predictive factors affecting postoperative quality of recovery for patients undergoing surgery. IOSR J Nurs Health Sci 6: 50-60.
[Crossref], [Google Scholar]
- Ali H (2022) How long does it take to recover from joint replacement?
- Lugade V, Klausmeier V, Jewett B, Collis D, Chou LS (2008) Short-term recovery of balance control after total hip arthroplasty. Clin Orthop Relat Res 466: 3051-3058.
[Crossref], [Google Scholar], [Indexed]
- Jahic D, Omerovic D, Tanovic AT, Dzankovic F, Campara MT (2018) The effect of prehabilitation on postoperative outcome in patients following primary total knee arthroplasty. Medical Archives 72: 439-443.
[Crossref], [Google Scholar], [Indexed]
- Obermeier MC, Sikka RS, Tompkins M, Nelson BJ, Hamilton A, et al. (2018) Examination of early functional recovery after ACL reconstruction: Functional milestone achievement and self-reported function. Sports Health 10: 345-354.
[Crossref], [Google Scholar], [Indexed]
- Tekin AÇ, Saygili MS, AdaÅ? M, Çabuk H, Arslan SM, et al. (2016) Outcome of type 3 open tibial diaphyseal fractures managed with a limb reconstruction system: Analysis of a 49-patient cohort. Medical Principles and Practice: International Journal of the Kuwait University 25: 270-275.
[Crossref], [Google Scholar], [Indexed]
- Goyal S, Naik MA, Tripathy SK, Rao SK (2017) Functional outcome of tibial fracture with acute compartment syndrome and correlation to deep posterior compartment pressure. World J Orthop 8: 385-393.
[Crossref], [Google Scholar], [Indexed]

Open Access Journals
- Aquaculture & Veterinary Science
- Chemistry & Chemical Sciences
- Clinical Sciences
- Engineering
- General Science
- Genetics & Molecular Biology
- Health Care & Nursing
- Immunology & Microbiology
- Materials Science
- Mathematics & Physics
- Medical Sciences
- Neurology & Psychiatry
- Oncology & Cancer Science
- Pharmaceutical Sciences